Lung Surgeries

“Our mission is to deliver excellence through quality, patient-centred, compassionate care.”
Dr Sylvio Provenzano
MD, MSc, FRACS
Cardiothoracic Surgeon
Lung and Thoracic Surgery
Any surgery is reserved to treat conditions when other non-invasive methods are not possible or don’t provide good results. Generally speaking, surgery has two main objectives: to save lives (also know as ‘for prognosis’) and/or to improve or relieve symptoms. In regards to Thoracic Surgery, there are few reasons why a procedure can be indicated:
- Curative – That’s when the goal of the surgery is to cure the patient from the disease. For example, a lobectomy or a pneumonectomy to resect early-stage lung cancer.
- To Diagnose or Stage a Disease – When a tissue sample is needed to diagnose a disease, sometimes surgery is indicated to obtain this sample. For example, a wedge resection to determine if a nodule within the lung is cancer or not; a mediastinoscopy to sample nodes within the mediastinum and stage the cancer.
- Supportive – A surgery is considered supportive when it is performed to assist other forms of treatment. For example, the insertion of a tunneled venous access (portacath) to deliver chemotherapy or other drugs.
- Palliative – Such surgeries are performed to reduce symptoms without addressing the cause or cure the disease. For example, a pleurodesis to decrease fluid to build in the chest.
- Debulking – This is also known as cytoreductive surgery and is performed when a large mass is interfering with other organs. The mass is resected as much as possible but there is no curative intent. For example, when a large mass in the chest is pressing on the airway or the heart, debulking can be indicated to relieve those organs.
- Reconstructive – This is also considered as plastic surgery and is performed to improve appearance of a deformity without affecting symptoms or prognosis. For example, repair of pectus scavatum, also known as sunken or funnel chest.
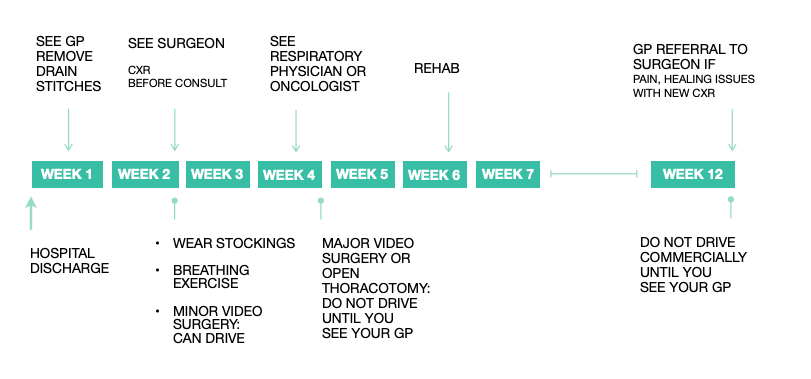
Your Journey
Typical Timeline after Hospital Discharge from Lung Surgery
U-VATS – Uniportal Video Assisted Thoracoscopic Surgery
Video-assisted thoracoscopic surgery or ‘VATS’ is any thoracic surgery whereby a camera is used to provide visualization. The camera and instruments are passed into the pleural space (space between the lung and chest wall) through holes in the chest wall, also called ports. Most procedures are performed through a single hole, hence Uniportal VATS – although more ports might be necessary.
U-VATS is a evolution in thoracic surgery, allowing for almost all types of surgery in the chest to be performed in a way that is safe and probably causes less pain than other methods (e.g. VATS with multiple ports or robot surgery). Click here to read what thoracic surgeons think of Uniportal VATS.
Small procedures such as pleural and lung biopsies, pleurodesis and pulmonary decortication are performed almost exclusively via U-VATS. VATS is also employed in the majority of larger resections such as lobectomies and resection of mediastinal tumors. [read more]
During the procedure, the lung and chest wall are inspected. The planned surgery then takes place. One or two drains and at times, a catheter for injection of local anaesthetic are inserted at the end of the procedure. The ports are closed with glue or stiches.
Sometimes it is not possible to complete the planned surgery via VATS due to abnormal anatomy, adhesions, too big tumor or bleeding. In these cases, Open Thoracotomy is necessary.
Open Thoracotomy – Open Surgery
Thoracotomy is the name of the incision through which thoracic surgery is performed. A cut is made at the front, side and/or back of the chest – according to the disease’s location.
The ribs are spread to access the chest cavity. Sometimes part of a rib or a whole one may be removed to improve visualization or decrease pain. The planned operation is performed.
One or two drains and at times, a catheter for injection of local anaesthetic are inserted at the end of the procedure. The chest wall is closed with stiches.
Sternotomy – Division of the Breastbone
Sternotomy is the name of the incision located in the middle of the chest, dividing the breastbone. It gives access to the thymus, the mediastinum, the great vessels and the heart. This incision is used in thoracic surgery mainly to resect tumours located anteriorly in the chest, such as thymomas, mediastinal cysts and masses.
The breastbone is closed with stainless steel wires or titanium plates. They will remain in your bone and should not activate metal detectors.
Common Thoracic Surgeries
- Pleural Biopsy – removal of small pieces of the lining of the pleural space.
- Pleurodesis – spraying of sterile talc powder into the pleural space or removal of the pleura lining of the chest wall.
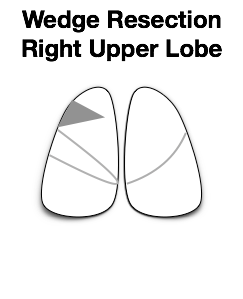
- Wedge Resection/Lung biopsy – removal of a piece of lung.
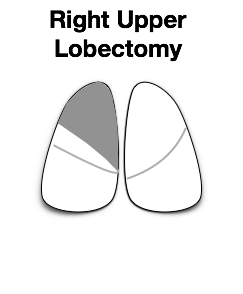
- Lobectomy – removal of large portion of lung (called ‘ lung lobe’).
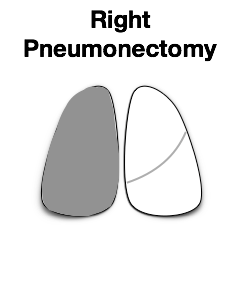
- Pneumonectomy – removal of the whole lung.
- Thymectomy – resection of the thymus gland.
- Exploratory Thoracotomy – to inspect and/or fix a condition within the chest cavity. For example, to control bleeding or to remove a clot or a tumor.
- Mediastinoscopy – performed via a small incision on the neck or chest wall. It is performed to obtain tissue biopsy for diagnosis or staging of lung cancer.
Associated Risks
As with any medical procedure, in a small number of cases, complications (adverse events) may occur. A large portion of the problems are consequences of previous conditions such as smoking, use of blood thinners, atherosclerosis, diabetes, previous diseases like stroke, heart, lung or renal failure, amongst others. It is fair to say that there are risks associated with the procedure and to the individual patient.
Cancer can recur independently of staging.
The risk of wound infection, chest infection, heart and lung complications and thrombosis increases with obesity and smoking.
Please speak to Dr. Provenzano regarding your individual circumstances and any questions or doubts you may have.
For information about associated risks of lung and thoracic surgery, please click here.
For an appointment or seeking a second opinion with Dr Provenzano, please contact:
Gold Coast Private Specialist Suites 14 Hill Street, Southport
P: (07) 5699 8258 F: (07) 5676 6784
Dr Sylvio Provenzano
MD, MSc, FRACS
Opening Hours
Gold Coast Private Specialist Suites